
The Fels Longitudinal Study was founded in Yellow Springs, Ohio, in 1929 as part of the Fels Research Institute. At that time, the Fels Longitudinal Study was one of five similar studies that began in the United States between 1927 and 1932. The Fels Study was originally designed to study child growth and development. Physical growth, maturation and the psychological development of children were early key research areas of interest in the Fels Longitudinal Study. Later, the Fels Longitudinal Study focused on physical growth, skeletal maturation, body composition, risk factors for cardiovascular disease and obesity, skeletal and dental biology, longitudinal biostatistical analyses and aging. In 1977, the Fels Research Institute and the Fels Longitudinal Study became part of the Wright State University’s Boonshoft School of Medicine, residing first in the Department of Pediatrics and later within the later the Department of Community Health (now the Department of Population & Public Health Sciences) in its Lifespan Health Research Center. The Fels Longitudinal Study was the longest operational longitudinal study of its kind in the world.
The original location of the Fels Longitudinal Study was Yellow Springs, Ohio, because in 1929, Arthur Morgan, then president of Antioch College in Yellow Springs, posed the question, "What makes people different?". He approached Samuel Fels, a Philadelphia businessman and philanthropist, regarding not only this question, but his idea that a longitudinal study from birth to adulthood would be required to answer to this question. Mr. Fels gave Morgan the backing needed to begin the study, and Lester W. Sontag M.D., Antioch College’s physician, was appointed the first director of the Fels Longitudinal Study in 1929. The first participants were enrolled prenatally by their parents, and the first examinations began in 1930. Dr. Sontag remained active in the study, developing, nurturing and guiding it until his retirement in 1970.
The Fels Research Institute was owned and operated by the Fels Fund of Philadelphia, a fund set up by Samuel Fels to continue his philanthropic endeavors. By the 1950s, the Fels Institute was also receiving additional support from the U.S. government from grants and contracts through the National Institutes of Health. In 1977, the Fels Fund donated the Institute to Wright State University School of Medicine, and the Institute was absorbed into the School of Medicine.

The original design of the Fels study called for the Fels participants to be enrolled into the study during the pregnancy of the mother, with the first measurements taken at or near the time of birth. Between 10 and 20 participants were enrolled each year. Some of the first mothers also became pregnant again, and their subsequent children, the siblings to the first participants, were also enrolled into the study. Over the years, as these first participants reached adulthood and started to have their own children, many of these second generation children were also enrolled. Eventually most of their children, grandchildren and great-grandchildren became dedicated Fels participants.
The dedication of Fels Longitudinal Study participants generated a wealth of significant health knowledge that has benefitted the people of the United States and of the world. One of the very first scientific papers on the effects of smoking on the fetus was published in 1936 using Fels data. The United States pediatric growth charts from 1978 to 2000 for children from birth to 3 years of age were produced exclusively from Fels data. The only valid method of measuring skeletal maturation (biological age) of U.S. children was developed using Fels data.
The Fels data set has been transferred to The University of Texas, Health Science Center at Houston (UTHealth), School of Public Health. Drs. Miryoung Lee and Stefan Czerwinski are the new stewards of the collection.
Researchers interested in working with the collection should contact Dr. Czerwinski at stefan.a.czerwinski@uth.tmc.edu.
Questions regarding participation in the study should be directed to Ms. Karla Akin at 937-999-5595 or Dr. Lee at miryoung.lee@uth.tmc.edu.
During a body composition visit, many methodologies are employed to obtain data on various functions and characteristics comprising the "body composition" of our participants. Below is a brief description of the types of samples taken and outcomes observed in the numerous methodologies involved during such a body composition visit. All methodologies are performed on a pre-determined schedule for those Fels Longitudinal Study participants consenting to participate in that portion of the testing. For a more detailed description of any of the methodologies described below, follow the appropriate link.
Anthropometry, the measurement of body parts, is completed on all participants at a variety of ages and growth ranges. Circumferences, bone breadths, lengths, weights and skinfolds are measured and recorded for various regions on each individual. Techniques in anthropometry and anthropometry for the elderly have been an area of interest for the Lifespan Health Research Center's staff.
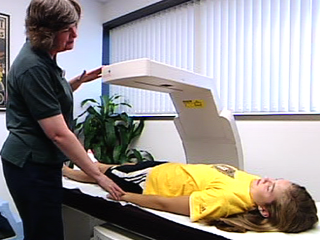
Dual energy x-ray absorptiometry (DXA) is performed on participants who fit the height and weight parameters of the Lunar densitometer. By scanning different anatomical regions, total body as well as segmented determinations may be made for, among other variables, bone mineral content, bone mineral density, muscle mass and percent of body fat.

Leanness, or specifically the amount of fat free mass, as well as total body fat and percent body fat is measured through the use of underwater weighing. In order to precisely calculate the amount of fat free mass, the lung residual volume is calculated to determine the volume of trapped air at maximal expiration. The amount of trapped air in the lungs adds more "float" to the individual, simulating increased body fat.
Bioelectrical impedance testing is performed in order to determine the amount of various body fluids as well as a measure for leanness. Electrodes are placed upon hands and feet and a small electrical current is passed through the body.
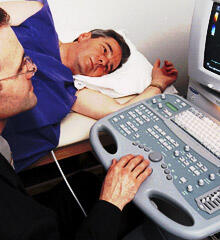
Measurements for subcutaneous fat is made through the use of ultrasound. Ultrasound is performed and measured on participants at 5 key sites on the body. Subcutaneous fat is also measured through the anthropometry portion of the testing.
Total body water is determined by the method of deuterium oxide (D2O) dilution. Deuterium is a non-radioactive naturally occurring molecule of water. The hydrogen atoms in deuterium are heavier than those that normally combine with oxygen to form water. Saliva samples are collected before other testing begins to establish a baseline measure of deuterium in the saliva. An amount of pure D2O is weighed, measured, and added to de-ionized water which is given to participants to drink. After a two hour fast and no urine eliminations, another saliva sample is taken and the amount of D2O remaining in the saliva is measured.

Fasting blood samples are collected on participants by a venous draw. From these samples levels of glucose, total cholesterol, triglycerides, high density lipoprotein cholesterol (HDL-C), low density lipoprotein cholesterol (LDL-C), and the apolipoproteins A1, A2, and B are observed. Samples are also taken to determine the levels of the hormones DHEA SO4, estradiol, free testosterone, total testosterone, and insulin within participants between the ages of 8 and 18 and in females over 40. Since estradiol levels fluctuate during the menstrual cycle, we attempt to collect estradiol samples on day 21 ± 3 of the menstrual cycle in those not taking oral contraceptives and on day 14 ± 3 of the cycle of those taking oral contraceptives.
Blood pressure is monitored and recorded on all participants. Grip strength on both hands is recorded.
Hand radiographs of the participants from age 8 through 18 are also taken. These radiographs are assessed to determine the skeletal ages of the individual and are scored through various established skeletal maturation assessment procedures.
Other data is also gathered through the use of questionnaires. Surveys are filled out by the participants to find out medical history, physical activity, tobacco and alcohol use, sexual maturity, and for females, menstrual history. For each visit, the participant fills out the relevant forms, updating us on this information.
The Fels data set has been transferred to The University of Texas, Health Science Center at Houston (UTHealth), School of Public Health. Drs. Miryoung Lee and Stefan Czerwinski are the new stewards of the collection.
Researchers interested in working with the collection should contact Dr. Czerwinski at stefan.a.czerwinski@uth.tmc.edu.
Questions regarding participation in the study should be directed to Ms. Karla Akin at 937-999-5595 or Dr. Lee at miryoung.lee@uth.tmc.edu.
Anthropometry

Anthropometric data can include weight, stature, sitting height, trunk depth, circumferences of the midarm, abdomen, hip, mid-thigh and maximum calf and triceps, biceps, subscapular, midaxillary, suprailiac, mid-thigh and lateral calf skinfold thicknesses. All measurements are taken using techniques similar to corresponding measurements in the Anthropometric Standardization Reference Manual (Lohman, T., Roche A., Martorel, R., eds., 1988, Human Kinetic Books) or to corresponding measurements in NHANES III. All measurements are taken by two independent observers, and measurements repeated if the initial measurement difference between the observers is greater than a preset error limit. Anthropometry has been collected continuously in the Fels Longitudinal Study since 1929.
Dual energy x-ray absorptiometry (DXA)
Total and regional body composition and bone density measurements are made using a dual energy x-ray absorptiometry or DXA. The information from a total body scan includes total body bone mineral (TBBM), soft-tissue, fat and lean tissue weights, and percent fat for 9 body regions (head and neck, left and right thorax, para-spinal, pelvis, each arm, each leg), as well as, total body fat (TBF), percent body fat (%BF), fat free mass (FFM), and TBBM. In addition, a lumbar spine and hip scan is performed for participants over 50 years of age. The precision for in vivo measurement of TBBM has been reported as 0.5 percent and that of estimates of %BF for the body regions and for the whole body is less than 1.5 percent. DXA has been used in the Fels Longitudinal Study since 1990.
Residual volume
Residual volume is measured on a Gould 2100 computerized lung function analyzer. Residual volume of each participant is measured twice, and the mean value is used in the body density calculations. Residual volume has been in use since 1977.
Ultrasound
Ultrasonic measurements of subcutaneous tissue are made at five sites: triceps, mid-thigh, suprailiac, paraspinal, and sacral using a Shimasonic SDL-32. Ultrasound transmission gel is placed upon each site and a 5 MHz transducer is used to acquire the images which are printed on a Mitsubishi video copy processor. Repeated images are made at each site, and the subcutaneous thicknesses are measured.
Grip strength and blood pressure
Grip strength is measured at each examination using a Lafayette hand dynamometer. Systolic and fourth and fifth phase diastolic blood pressures are measured seated by specially trained observers in a rigorously standardized manner. Blood pressure data have been collected since the early 1930s.
Skeletal maturation
In the longitudinal growth study many asessments made of participants are measures of maturation. Skeletal maturation involves the changes in the bones as an individual becomes an adult. This has been an area of interest in the Fels Longitudinal Study for most of the history of the study. The FELS Method for assessing the skeletal age of the hand-wrist was developed in the 1980s. Hand-wrist x-rays are taken from most participants between ages 8 and 18 years. Skeletal age can differ in two children of the same chronological age and stature and still be normal.
Health history, menstruation, smoking, alcohol, function and physical activity
Demographic information and a comprehensive health history questionnaire are collected from participants at each examination. These data are used to help describe possible confounding interactions and associations within the data. Habitual physical activity is estimated for previous year and previous day using modified Baecke questionnaires to categorize participants by calculating a total activity score from work, sports, and non-sports leisure time activity indices.
At each examination, the participant is given a series of questionnaires to complete which include an interval medical history (a five-page, detailed inquiry of current health status including chronic, acute and infectious conditions), physical activity (a two-page detailed inquiry relating to frequency, intensity, duration and type of exertion spent in work and leisure activities), tobacco and alcohol use (a four-page inquiry relating to current alcohol, tobacco and drug usage or exposure), and a menstrual history (three two-page inquires depending upon the age of the women relating to gynecological health and status and supplemental hormone use). The tobacco and alcohol forms include questions about smokeless tobacco and exposure to environmental smoke. The SF-36 is used to assess function and wellbeing for participants 60 years and older. The SF-36 is an accepted and validated assessment tool for measuring a comprehensive set of defined health concepts applicable to the aging process. Maturity is assessed in children by self-administered questionnaires reflecting pubic hair development and genital development. Health, menstrual and behavior data have been collected in the Fels Longitudinal Study since 1929. Physical activity data have been collected since 1988.
The Fels data set has been transferred to The University of Texas, Health Science Center at Houston (UTHealth), School of Public Health. Drs. Miryoung Lee and Stefan Czerwinski are the new stewards of the collection.
Researchers interested in working with the collection should contact Dr. Czerwinski at stefan.a.czerwinski@uth.tmc.edu.
Questions regarding participation in the study should be directed to Ms. Karla Akin at 937-999-5595 or Dr. Lee at miryoung.lee@uth.tmc.edu.